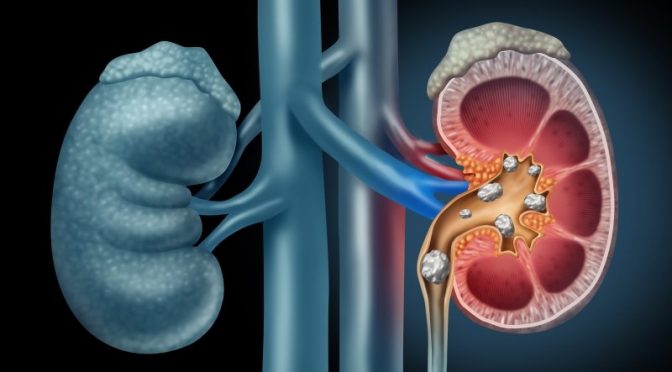
Kidney stones are hard, crystalline mineral and acid deposits which form in the kidney or urinary tract. They are sometimes called renal calculi. It is possible for anyone to develop a kidney stone. However, certain diseases and conditions or those who are taking certain medications are more prone to this formation.
Kidney stone disease is the most painful urological disorder. Humans have been suffering from this disorder for centuries. Scientists have found evidence of kidney stones in a 7,000-year-old Egyptian mummy.
The incidence of urolithiasis, or stone disease, has increased in the last 25 years. The reasons for this are dietary and climatic changes. Kidney stones are most common in middle-aged people and are 3 times more common in men than in women.
Urbanisation, stress at work and change in food habits are some of the conditions attributed to the increase in the incidence of stone diseases of late.
Risks of developing stones
- Drinking less fluid
- Diet with low calcium, high animal protein, high sugars and high sodium
- Use of calcium supplements
- Obstruction to urine outflow like in prostate enlargement or stricture disease
- Hyperparathyroidism (an endocrine disorder that results in more calcium in urine)
- Gout
- Obesity
- Chronic diarrhoea
- Family history
Causes
- More calcium, oxalate or uric acid in stones due to metabolic disorder, gout, intestinal bypass surgery or genetic factors
- Repeated urinary tract infections
- A family history can be an important factor in kidney stones. They are more common in Asians and Caucasians than in Native Americans, Africans or African Americans.
- A subset of kidney stones, uric acid kidney stones are more common in people with chronically elevated uric acid levels in their blood.
- Even pregnancy can sometimes factor in the formation of kidney stones. The reason for this is that the passage of urine slows down in the woman due to increased secretion of the progesterone hormone. To add to this, the enlarged uterus results in a lower bladder capacity during pregnancy. This then leads to lower fluid intake which further aggravates the situation.
- Dehydration from reduced fluid intake or strenuous exercise without necessary fluid replacement increases the risk of kidney stones.
Symptoms
The symptoms depend upon where the stone is located
- If the stone is in the kidney: dull aching continuous pain in the loins, repeated urinary tract infections or sometimes intermittent blood in the urine, especially in a young adult
- If the stone is in the ureter: Stones usually at least 3 mm can cause obstruction of the ureter. Ureteral obstruction causes hydronephrosis (distension and dilation of the renal pelvis and calyces) as well as spasm of the ureter. This leads to pain, most commonly felt in the flank (the area between the ribs and hip), lower abdomen and groin (a condition called renal colic). Renal colic can be associated with nausea, vomiting, sweating, urinary urgency, blood in the urine and painful urination. Renal colic typically comes in waves lasting from minutes to hours, beginning in the flank or lower back and often radiating to the groin or genitals. It is caused by contractions of the ureter as it attempts to expel the stone.
- Sometimes patient presents with lithuria : eliminating gravel or stones while passing urine
- Sometimes they are asymptomatic, especially when it is present in the kidney. A large kidney stone shaped like a like stag horn which occupies more than 80% of the kidney may not produce any symptoms and come to light when undergoing evaluation for some other diseases.
How is it diagnosed?
Diagnosis is made on the basis of:
- Clinical findings
- X- ray of abdomen
- Ultrasonography
- Urine examination
- Sometimes advanced tests like spiral CT or contrast CT may be required.
Is recurrence common even after complete removal of stones?
- Stone recurrence is very common. If not treated, there is a 20-30% chance that it recurs within 2 years, 50% chance within 5 years and 65% chance in 10 years.
- If treated appropriately with diet modifications to reduce the stone formers in the body, chances of recurrence can be reduced.
What are the complications of stone disease?
- Repeated infection / pyelonephritis etc.
- Obstruction may lead to temporary kidney failure with rise in serum creatinine.
- If obstruction is repeated and not treated, especially in those with other associated systemic diseases, it might lead to permanent renal failure needing dialysis and renal transplant.
- Renal failure i.e. chronic kidney diseases
Treatment
Medical management: for those who pass small stones in urine or are asymptomatic. These patients should undergo complete investigations, blood and urinary metabolic evaluation to find out the cause and be treated.
Surgery: These are patients who have stones causing obstruction, repeated infection and malfunctioning of the kidneys. These patients may require early surgical intervention to prevent complications.
Surgery options
- Extracorporeal shock wave lithotripsy (ESWL): for the moderate sized soft stone located in the kidney or ureter where the stone is fragmented using a lithotriptor via the shockwave delivered from outside the body. The main advantage is that the procedure can be done in an outpatient setting.
- Endoscopic removal for the stones in the lower ureter
- Flexible ureteroscopy and laser disintegration for the stones in the complex inaccessible part of the urinary system
- Percutaneous nephrolithotomy (PCNL) for the large stones of the kidney
- Laparoscopic method is often used to treat complex pelvic stones.
- Open surgery in selected cases
Surgical treatment of stones includes:
- Shock wave lithotripsy (ESWL)
- Ureteroscopy (URS)
- Retrograde intrarenal surgery (RIRS)
- Percutaneous nephrolithotomy (PCNL)
- Laparoscopic or open surgery
Semi rigid ureteroscopyThis is an endoscopic method where a miniature (6 fr) scope is passed through the urethra and the stones are fragmented and removed under direct vision. This method is commonly used for the removal of stones when they are present in the mid and lower ureter and sometimes for the large upper ureteric stones. In this method, the stone is directly visualised and broken with pneumatic or ultrasonic lithotripsy or using laser. The main advantage is complete stone clearance in a single stay.
Retrograde intra renal surgery(RIRS)
This is an advanced endoscopic technique of fragmenting the stone in situ using a flexible ureteroscope and laser. Here, the stone is approached anywhere in the calyces of the kidney. Most of the complex small stones in the kidney can be tackled by this method. It is one of the most favoured approaches for stone treatment currently.
Percutaneous nephrolithotomy (PCNL):
Here, the kidney is directly punctured through the skin and a tract is made to approach the stone. Then the endoscope (nephroscope) is used to visualise the stone and is fragmented by the available energy sources and laser. This method is useful in large stone bulk within the kidney. Patient needs to stay in the hospital for 4-5 days.
Laparoscopic / open-stone removal
Open surgery: because these procedures are the most invasive and painful, patients often spend up to 5-7 days in the hospital. Complete recovery may take up to six weeks. Present day indications for open surgery for stone removal are only 2%.
This procedure is replaced by minimally invasive laparoscopic method. Here, the stone is removed via a keyhole surgery technique. Most of the stones can be removed effectively by laparoscopic methods. Laparoscopy has the advantage of minimal scarring, less pain, immediate recovery and early return to work.


0 Comment